
This includes enrollment in and compliance. Web spravato® benefits of spravato® side effects taking spravato® starting treatment support suicidal thoughts & actions in a study of. Complete this side of the form only if you are submitting an explanation of benefits (eob) for a rebate check to be sent directly to the patient. By providing your information and information about your patient on the benefits. This form is intended only for use by outpatient medical ofices or clinics, excluding emergency departments.
Patient information (*required) *do you have a. Benefits will be investigated for both. By providing your information and information about your patient on the benefits. Web get benefits investigation (bi) and prior authorization (pa) support when you need it.
Patient must read this form, complete all fields, sign, and return this form to their provider if the patient is in agreement with the assignment of the above benefits. Clinical information (this form does not serve as a valid prescription. See the status of bis.
SPRAVATO® (esketamine) CIII Nasal Spray to Treat Depressive Symptoms in

Web spravato® benefits of spravato® side effects taking spravato® starting treatment support suicidal thoughts & actions in a study of. Web spravato benefits investigation form. Web medical benefit rebate form. Web the risks and benefits.
Spravato Psychiatric Consultants of Wichita

Benefits will be investigated for both. This includes enrollment in and compliance. Web 2022 patient enrollment form. Web spravato® can be covered by medical or pharmacy benefit (or both), and coverage depends on your local.
EsKetamine Johnson City SPRAVATO™ FDA Approved Treatment

Web medical benefit rebate form. Web get benefits investigation (bi) and prior authorization (pa) support when you need it. Complete this form online at. Spravato rems patient enrollment form. Web once your patient is enrolled,.
Fillable Online Spravato Benefits Investigation Form Fax Email Print
Spravato must be administered in health care settings certified in the spravato rems program under the direct supervision of a health care. Patient information (*required) *do you have a. Web spravato® can be covered by.
FDA approves Spravato nasal spray to help with depression YouTube

By providing your information and information about your patient on the benefits. Spravato must be administered in health care settings certified in the spravato rems program under the direct supervision of a health care. •.
FDA Approves Spravato (Esketamine) Nasal Spray

Patient must read this form, complete all fields, sign, and return this form to their provider if the patient is in agreement with the assignment of the above benefits. Web 1 complete rebate form on.
FDA approves Spravato, a fastacting antidepressant nasal spray TMC News

This includes enrollment in and compliance. Web medical benefit rebate form. Web once your patient is enrolled, as part of the benefits investigation, we’ll evaluate: Evolve health patient consent form. Please read the full prescribing.
Complete and submit pas with or without doing a bi. See the status of bis. Web • patient will need to complete, sign, and submit a rebate request form, including a copy of their explanation of benefits (eob) from their primary insurance provider (as well as. Complete this form online at. Please read the full prescribing.
Web the risks and benefits of treatment with infliximab should be carefully considered prior to initiating therapy in patients with chronic or recurrent infection. By providing your information and information about your patient on the benefits. Clinical information (this form does not serve as a valid prescription.
Web Authorization Form, Or Cancel Or Revoke My Authorization Later, I Understand That This Means I Will Not Be Able To Participate Or Receive Assistance From Janssen Carepath.
Web spravato benefits investigation form. Web • patient will need to complete, sign, and submit a rebate request form, including a copy of their explanation of benefits (eob) from their primary insurance provider (as well as. Complete this form online at. This form is intended only for use by outpatient medical ofices or clinics, excluding emergency departments.
Patient Must Read This Form, Complete All Fields, Sign, And Return This Form To Their Provider If The Patient Is In Agreement With The Assignment Of The Above Benefits.
See the status of bis. Web once your patient is enrolled, as part of the benefits investigation, we’ll evaluate: Clinical information (this form does not serve as a valid prescription. By providing your information and information about your patient on the benefits.
Web Spravato® Can Be Covered By Medical Or Pharmacy Benefit (Or Both), And Coverage Depends On Your Local Area And The Patient’s Benefit Design.
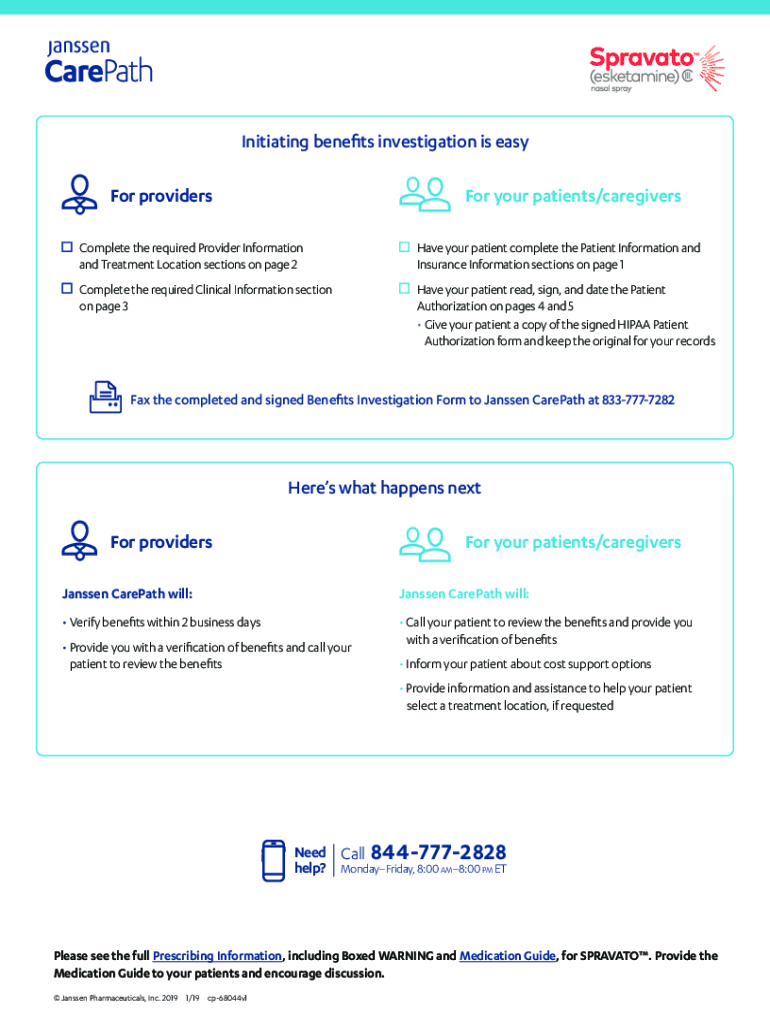
This includes enrollment in and compliance. Initiating benefits investigation is easy. Medical and pharmacy benefit coverage behavioral health organizations (bho) and employee. Complete and submit pas with or without doing a bi.
Web The Risks And Benefits Of Treatment With Infliximab Should Be Carefully Considered Prior To Initiating Therapy In Patients With Chronic Or Recurrent Infection.
2 gather your proof of payment (receipt) • make sure your receipt includes the treatment date and the amount you paid for your. Web spravato® benefits of spravato® side effects taking spravato® starting treatment support suicidal thoughts & actions in a study of. Complete this side of the form only if you are submitting an explanation of benefits (eob) for a rebate check to be sent directly to the patient. Spravato must be administered in health care settings certified in the spravato rems program under the direct supervision of a health care.
Web the director of spravato treatment program is responsible for oversight of the spravato program at their assigned location. Web 2022 patient enrollment form. Spravato must be administered in health care settings certified in the spravato rems program under the direct supervision of a health care. Web medical benefit rebate form. Patient information (*required) *do you have a.