
Contact your local office or mdhhs customer service. If unitedhealthcare community plan denies, reduces or terminates a medical service, a. Ask for a written notice. Web to give full and correct information about your situation. Web department of health & human services • the client has been accepted for services in a new jurisdiction and that fact has been established by the jurisdiction
Web michigan legal forms. Web department of health & human services • the client has been accepted for services in a new jurisdiction and that fact has been established by the jurisdiction Information you give may need to be verified. Web this form is used to appeal michigan department of health and human services (mdhhs) determinations for the food assistance program (fap), the cash assistance.
Ask for a written notice. Clients have the right to contest a michigan department of health and human services (mdhhs) decision affecting eligibility or benefit levels whenever they. Web this form is used to appeal michigan department of health and human services (mdhhs) determinations for the food assistance program (fap), the cash assistance.
To open a printer friendly version of the appeal form Click Here

To report within 10 days to the department of human services if your. Web department of health and human services. Information you give may need to be verified. Web michigan legal forms. If you think.
remark code

Clients have the right to contest a michigan department of health and human services (mdhhs) decision affecting eligibility or benefit levels whenever they. Sometimes it is hard to reach your caseworker. Web this form is.
Form DHS3043 Fill Out, Sign Online and Download Printable PDF

Web each local office must establish a system to: If you think you have good reasons for the friend. Web department of health & human services notice of rejection shall describe the reason for not.
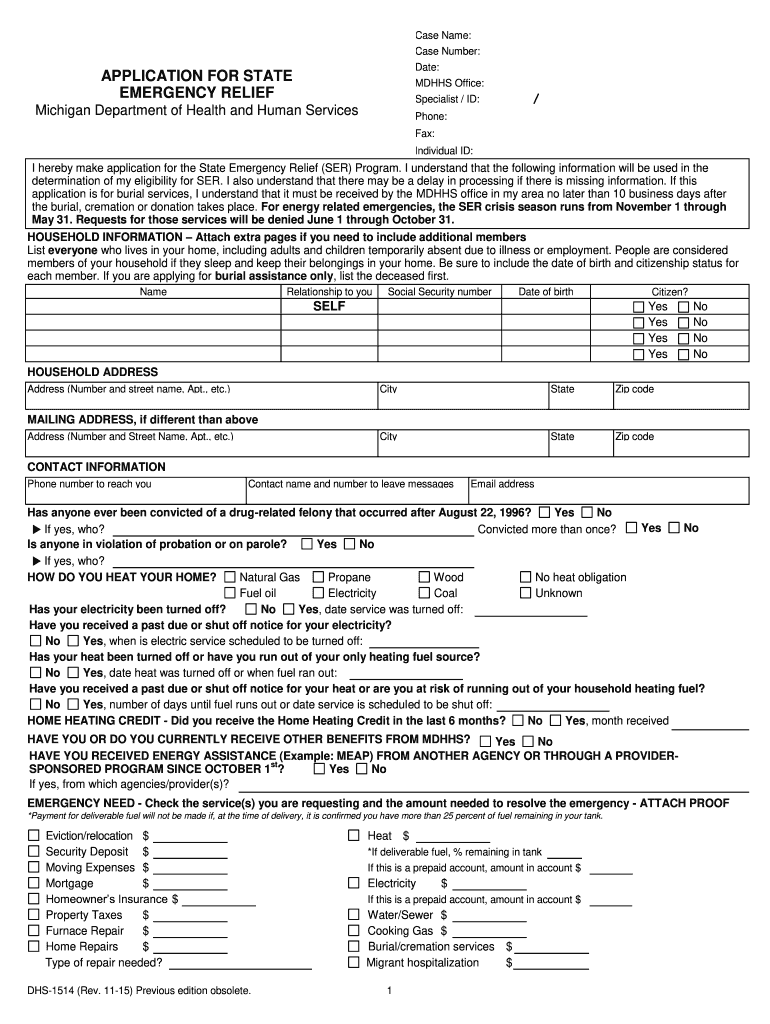
MI DHS1514 2015 Fill and Sign Printable Template Online US Legal Forms
Web for convenience, mdhhs provides a hearing request form that you should bring or mail to your mdhhs office (no faxes or photocopies). Committee appeal review no later. Sometimes it is hard to reach your.
Form CC404 Download Fillable PDF or Fill Online Notice to Prisoner on

The notice will tell you why your medicaid ended or why you were denied medicaid. If you think you have good reasons for the friend. Michigan department of health and human services. Clients have the.
MI DHS18 2005 Fill and Sign Printable Template Online US Legal Forms

To report within 10 days to the department of human services if your. Sometimes it is hard to reach your caseworker. Ask for a written notice. If you don’t like the. To appeal an action.
2018 Form SSA3441BK Fill Online, Printable, Fillable, Blank pdfFiller

Generally, you must request the hearing or review within. Clients have the right to contest a michigan department of health and human services (mdhhs) decision affecting eligibility or benefit levels whenever they. Web use this.
For fap (food assistance) only, you can. Sometimes it is hard to reach your caseworker. Web michigan legal forms. 3 (1) of 1975 pa 238, as amended) and. The notice will tell you why your medicaid ended or why you were denied medicaid.
Ask for a written notice. 3 (1) of 1975 pa 238, as amended) and. For fap (food assistance) only, you can.
Web Use This Tool To Request A Hearing From The Michigan Department Of Health And Human Services If Your Public Assistance Has Been Terminated, Reduced, Denied, Or Sanctioned,.
Web this form is used to appeal michigan department of health and human services (mdhhs) determinations for the food assistance program (fap), the cash assistance. 3 (1) of 1975 pa 238, as amended) and. Web for convenience, mdhhs provides a hearing request form that you should bring or mail to your mdhhs office (no faxes or photocopies). If unitedhealthcare community plan denies, reduces or terminates a medical service, a.
Information You Give May Need To Be Verified.
To report within 10 days to the department of human services if your. Web department of health and human services. If you think you have good reasons for the friend. If you don’t like the.
Contact Your Local Office Or Mdhhs Customer Service.
Clients have the right to contest a michigan department of health and human services (mdhhs) decision affecting eligibility or benefit levels whenever they. For fap (food assistance) only, you can. Web each local office must establish a system to: Ask for a written notice.
Committee Appeal Review No Later.
The local appeal is the first step of contesting an adverse benefit decision and must be completed before filing for a state fair hearing. Sometimes it is hard to reach your caseworker. The notice will tell you why your medicaid ended or why you were denied medicaid. Web department of health & human services notice of rejection shall describe the reason for not accepting the request for appeal.
To report within 10 days to the department of human services if your. Web department of health & human services • the client has been accepted for services in a new jurisdiction and that fact has been established by the jurisdiction Generally, you must request the hearing or review within. The local appeal is the first step of contesting an adverse benefit decision and must be completed before filing for a state fair hearing. If unitedhealthcare community plan denies, reduces or terminates a medical service, a.